

احتباس ادرار به دلیل دیسک کمر شرایطی است که زمانی ایجاد می شود که فتق دیسک در ستون فقرات کمر اعصاب مسئول کنترل عملکرد مثانه را تحت فشار قرار دهد.
ستون فقرات کمری شامل پنج مهره (L1-L5) است که در ناحیه کمر قرار دارند. بین این مهرهها دیسکهای بین مهرهای قرار دارند که به عنوان ضربهگیر عمل میکنند و باعث انعطافپذیری ستون فقرات میشوند. هر دیسک شامل یک لایه بیرونی سخت به نام حلقه فیبروزوس و یک هسته داخلی ژل مانند به نام هسته پالپوس است. نخاع در سطح مهره اول یا دوم کمری ختم می شود و ساختاری به نام مخروط مدولاریس را تشکیل می دهد. در زیر این سطح، اعصاب نخاعی به صورت دستهای از ریشههای عصبی به نام دم اسبی به سمت پایین گسترش مییابند.
فتق دیسک زمانی اتفاق میافتد که هسته داخلی دیسک از لایه بیرونی بیرون بزند، اغلب در نتیجه تغییرات دژنراتیو، ضربه یا فشار مکرر. فتق دیسک کمر معمولاً سطوح تحتانی کمر، به ویژه L4-L5 و L5-S1 را تحت تأثیر قرار می دهد، زیرا به دلیل افزایش استرس مکانیکی در این ناحیه است. When a disc herniates, it can compress nearby spinal nerves, including those that innervate the bladder.
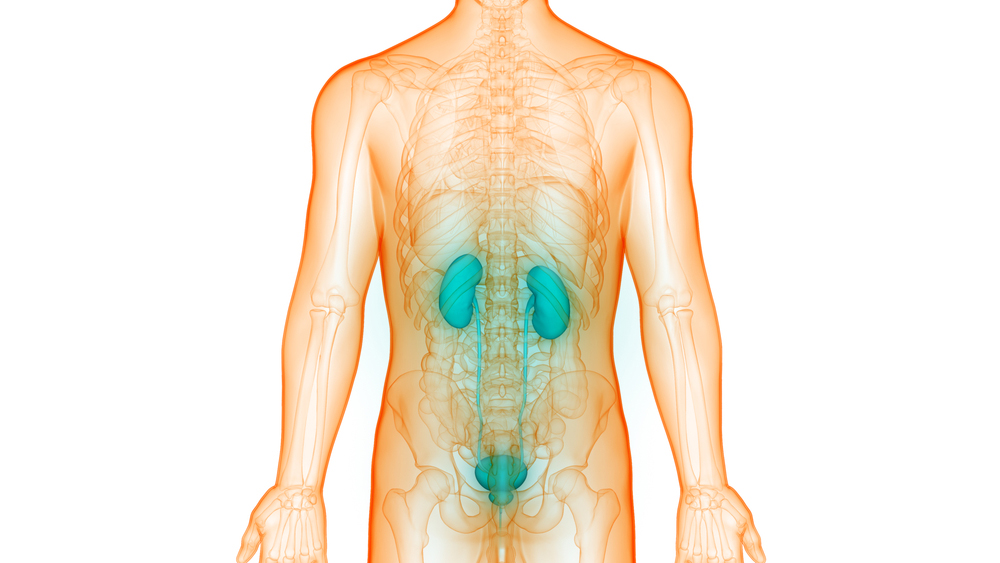
The bladder is a hollow muscular organ located in the pelvis that stores urine produced by the kidneys before excretion. This nerve is innervated by a complex network of nerves that regulate its functions, including the sensation of fullness, initiation of voiding, and coordination of bladder contraction and sphincter relaxation during urination. The primary nerves responsible for controlling the bladder originate from the sacral spinal cord (S2-S4) and form the pelvic nerves.
Symptoms of urinary retention due to lumbar disc
When a herniated lumbar disc compresses the nerves that control bladder function, it can disrupt the normal nerve signals needed for urination. The specific symptoms experienced by a person with urinary retention due to a herniated lumbar disc can vary depending on the severity and location of the nerve compression. However, common symptoms may include:
Difficulty starting to urinate: Compression of the nerves that are involved in starting bladder contractions can lead to difficulty starting to urinate, despite feeling the urge to urinate.
Poor urinary flow: Nerve compression may lead to weak bladder contractions, resulting in reduced urinary flow during voiding.
Incomplete bladder emptying: Due to nerve dysfunction, the bladder may not empty completely during urination, resulting in residual urine in the bladder.
Hesitancy in urination: People may hesitate or delay starting to urinate, even when they feel the urge to urinate.
Overflow incontinence: In severe cases of urinary retention, the bladder may become overfilled and unable to empty properly, resulting in involuntary leakage of urine.
Diagnosing urinary retention due to a herniated lumbar disc usually involves a comprehensive evaluation by a health care professional, including a detailed medical history, physical examination, and diagnostic tests. Imaging studies such as magnetic resonance imaging (MRI) can help identify the presence and location of a herniated disc and nerve compression in the lumbar spine. In addition, urodynamic studies may be performed to assess bladder function and identify any abnormalities in urine flow and bladder emptying.
treatment methods
Treatment options for urinary retention due to a lumbar disc are aimed at reducing nerve pressure, restoring bladder function, and relieving symptoms. رویکرد درمانی مناسب به شدت علائم، میزان فشرده سازی عصب و وضعیت کلی سلامت فرد بستگی دارد.
درمان های محافظه کارانه ممکن است شامل موارد زیر باشد:
استراحت و اصلاح فعالیت: اجتناب از فعالیتهایی که علائم را تشدید میکنند، مانند بلند کردن اجسام سنگین یا نشستن طولانیمدت، میتواند به کاهش فشار روی ستون فقرات کمری و کاهش فشار عصبی کمک کند.
داروها: داروهای ضد التهابی غیراستروئیدی (NSAIDs)، شل کننده های عضلانی و داروهای ضد درد ممکن است برای کاهش درد و التهاب مرتبط با فتق دیسک تجویز شوند.
فیزیوتراپی دیسک کمر: تمرینات هدفمند و تکنیک های کششی می تواند به تقویت عضلات حمایت کننده از ستون فقرات، بهبود وضعیت بدن و کاهش فشار روی اعصاب آسیب دیده کمک کند.
تزریق استروئید اپیدورال: تزریق کورتیکواستروئیدها به فضای اپیدورال اطراف ریشه های عصبی آسیب دیده می تواند به کاهش التهاب و کاهش علائم فشرده سازی عصب کمک کند.
کاتتریزاسیون: در موارد احتباس شدید ادرار که اقدامات محافظه کارانه بی اثر هستند، ممکن است از کاتترهای موقت یا ساکن ادرار برای تخلیه ادرار از مثانه تا بهبود عملکرد عصبی استفاده شود.
در مواردی که درمان های محافظه کارانه نمی توانند تسکین کافی را ارائه دهند یا علائم بدتر می شوند، مداخله جراحی ممکن است برای رفع فشار اعصاب آسیب دیده و کاهش احتباس ادرار در نظر گرفته شود.