
Inflammatory bowel diseases (IBD) include two main diseases Crohn and ulcerative colitis. Both cause chronic inflammation of the gastrointestinal tract, but the site of involvement, severity of symptoms, diagnosis and treatment method are not the same. بسیاری از بیماران سالها با علائمی مثل دلدرد، اسهال یا خونریزی روده درگیرند، اما نمیدانند کدام نوع IBD را دارند و چطور باید آن را مدیریت کنند.
در این مقاله، به زبانی کاملاً ساده و دقیق تفاوتهای اصلی کرون و کولیت اولسروز را توضیح میدهیم.
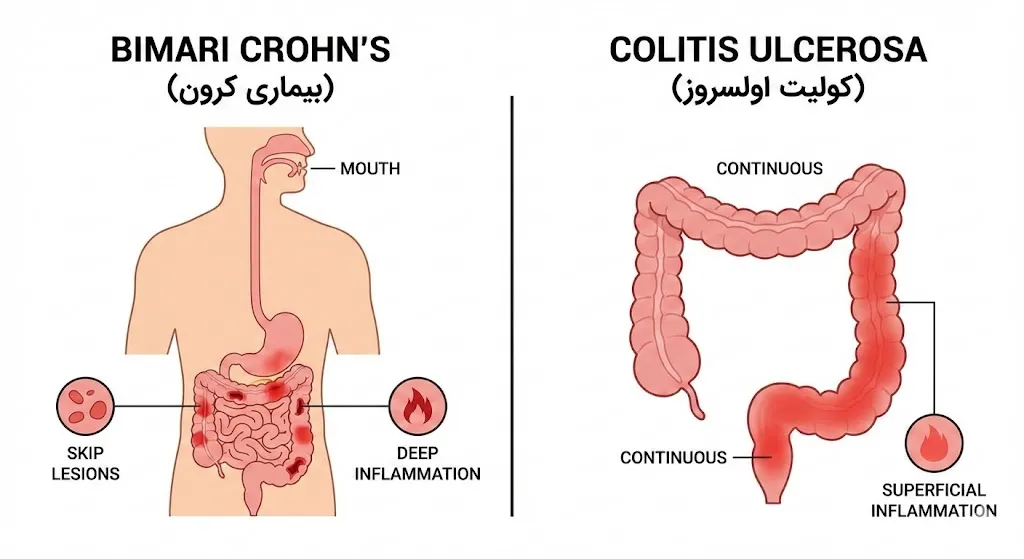
🟩 کرون چیست؟
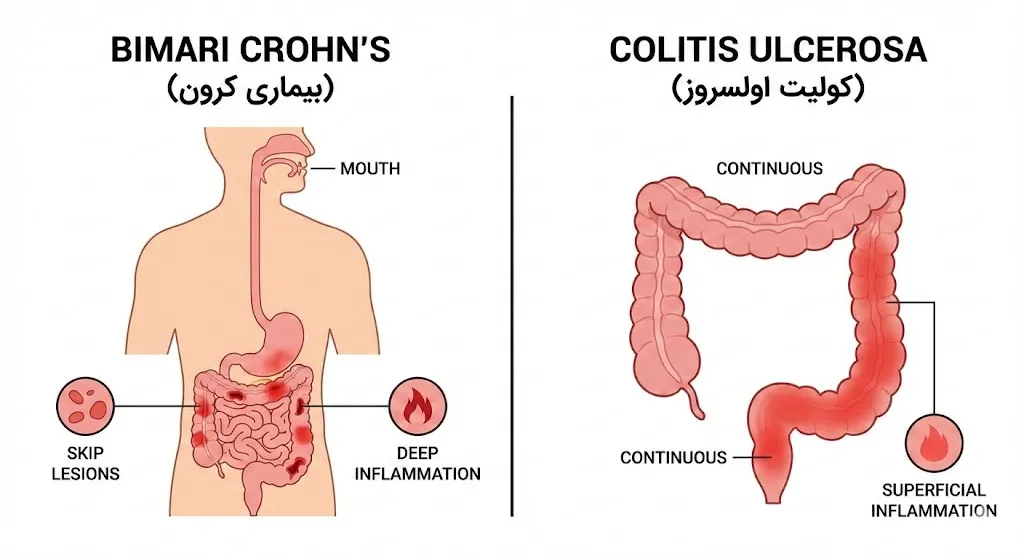
بیماری کرون (Crohn’s Disease) نوعی التهاب مزمن است که میتواند از دهان تا مقعد هر نقطهای از لوله گوارش را درگیر کند.
در کرون:
-
التهاب «لایهبهلایه» است
-
ممکن است باعث تنگی روده، فیستول و آبسه شود
-
اغلب بهصورت بخشهای سالم و بیمار پشتسر هم دیده میشود (Skip Lesions)
🟥 کولیت اولسروز چیست؟
کولیت اولسروز (Ulcerative Colitis) فقط روده بزرگ (کولون) را درگیر میکند و التهاب آن:
-
سطحیتر است (در لایه مخاط)
-
از رکتوم شروع میشود و به سمت بالا گسترش مییابد
-
پیوسته است (بدون بخشهای سالم و بیمار)
🟦 تفاوتهای کلیدی کرون و کولیت اولسروز
1) محل درگیری
| ویژگی | کرون | کولیت اولسروز |
|---|---|---|
| محدوده | از دهان تا مقعد | فقط روده بزرگ |
| الگوی درگیری | تکهتکه (Skip) | پیوسته |
2) شدت و عمق التهاب
-
کرون: التهاب عمقی → احتمال فیستول، آبسه، تنگی روده
-
کولیت: التهاب سطحی → خونریزی و اسهال خونی شایعتر
3) علائم رایج
🟩 علائم شایع کرون:
-
درد شکمی مزمن
-
کاهش وزن
-
اسهال طولکشیده
-
تب
-
تنگی روده یا انسداد
-
فیستول (مثلاً روده به پوست یا سایر اندامها)
🟥 علائم شایع کولیت اولسروز:
-
اسهال خونی
-
فوریت دفع
-
درد پایین شکم
-
احساس تخلیه ناکامل
-
التهاب رکتوم (پروکتیت)
🟦 چطور کرون و کولیت اولسروز تشخیص داده میشوند؟
تشخیص این دو بیماری معمولاً ترکیبی از موارد زیر است:
🔍 1) کولونوسکوپی و بیوپسی
دقیقترین ابزار تشخیص است.
در کولونوسکوپی:
-
الگوی التهاب
-
عمق زخمها
-
محل درگیری
به پزشک کمک میکند نوع بیماری را مشخص کند.
🧪 2) آزمایشهای خونی و مدفوع
برای بررسی:
-
التهاب سیستمیک
-
کمخونی
-
مارکرهای التهابی (CRP, ESR)
-
کالپروتکتین مدفوع
🖥 3) سیتی یا امآرای انتروگرافی
در کرون بسیار کاربردی است، چون درگیری روده باریک یا فیستولها را نشان میدهد.
🟦 آیا درمان کرون و کولیت اولسروز متفاوت است؟
درمان هر دو بر اساس کنترل التهاب و جلوگیری از حملات بیماری انجام میشود؛ But there are differences.
🟩 Crohn's treatment
-
Aminosalicylates
-
Corticosteroids
-
immunomodulators
-
Biologics (Anti-TNF, Anti-IL, Anti-integrin)
-
Severe cases: surgery to remove stenosis or fistula
Treatment of ulcerative colitis
-
Local and oral anti-inflammatory drugs
-
cortones
-
immunosuppressive drugs
-
Biologics
-
In very severe cases: Surgery and complete removal of the colon (definitive treatment)
🟦 Which one has the risk of cancer?
-
Ulcerative colitis in long-term colonic involvement → increases the risk of colon cancer
-
Crohn also has the same risk if the colon is involved, but usually less
Regular colonoscopy screening is an important part of managing these patients.
🟩 Which one is more intense?
None are "more severe"; Intensity to:
-
Site of conflict
-
Inflammation depth
-
Response to treatment
-
The lifestyle of the patient
It depends.
🟦 When should you see a specialist doctor?
If the following symptoms are present, you need to be evaluated quickly:
-
bloody diarrhea
-
Persistent abdominal pain
-
Unreasonable weight loss
-
Long fever
-
diarrhea for more than 4 weeks
-
Extreme urgency to dispose of
-
Family history of IBD
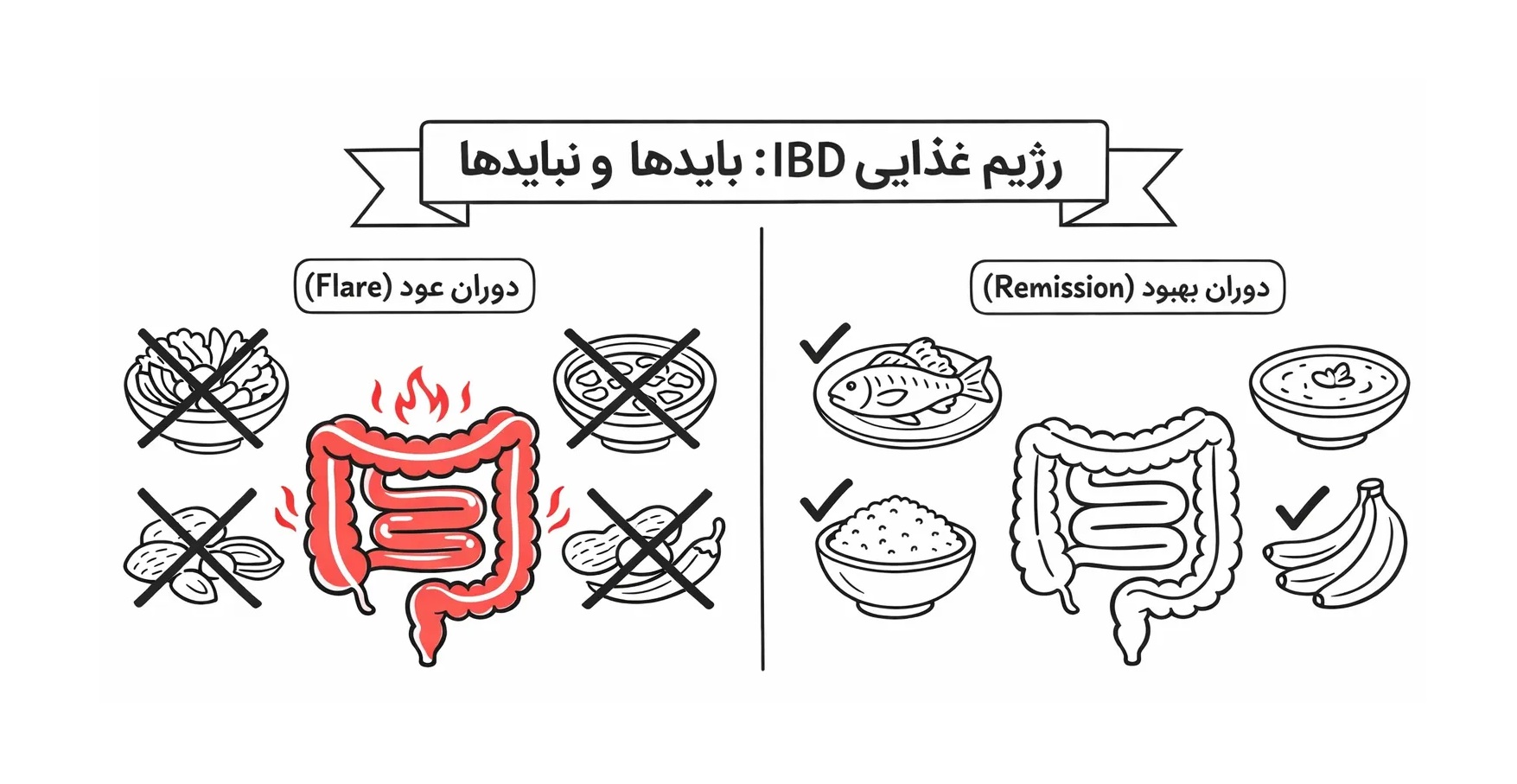
🟩 Summary in plain language
-
Ulcerative colitis → colon only, superficial inflammation, common dysentery
-
Crohn → any part of the digestive system, deep inflammation, possibility of fistula and intestinal stricture
-
Definitive diagnosis only with colonoscopy + imaging + tests
-
Their treatment is similar, but it is chosen depending on the type of disease and its severity
-
Careful and long-term management under the supervision of an IBD specialist produces the best results