

بارداری و IBD
اگه شما با Crohn’s disease یا Ulcerative colitis دست و پنجه نرم میکنید و قصد دارید بچه دار شوید، احتمالاً کلی سوال براتون پیش میاد. These questions may include the following:
Can I get pregnant?
Is pregnancy a condition of inflammatory bowel disease? Does it make me worse?
Can the disease or medicines I take harm the baby? After giving birth, will I be able to breastfeed?
Remember that each person's situation is different; Therefore, any decision you make, including pregnancy, should be made with the cooperation of gastroenterologists and obstetricians.
In the following, we review some general points about pregnancy and IBD in a friendly manner:
Pregnancy and IBD:
In general, women with Crohn's disease or ulcerative colitis who are in remission can get pregnant as easily as other women their age.
Women whose disease is active or who have had surgery in the pelvis, for example, they had a colectomy with a patch, may face more challenges in fertility.
For men, having IBD does not affect fertility; But some drugs like Sulfasalazine can affect the quality and number of sperm. If men are using this medicine, it is better to consult their doctor at the IBD specialist center. data-uniq-id="cekbg" data-generated-css="brz-css-qlkjn">Currently, until more studies are conducted, the use of ozanimod, ipadacitinib and tofacitinib during pregnancy is not recommended and should be replaced with other drugs. With IBD:
it is better to put the disease into remission before pregnancy;
pregnancy Start at the time of relapse or when a new treatment has just started. If your disease recurs during pregnancy, controlling it again can be problematic.
It is interesting that in some cases, pregnancy improves the disease; Because the body's immune system is slightly suppressed during this period to prevent rejection of the embryo. Studies have shown that pregnancy may prevent the recurrence of the disease in the future and reduce the need for surgery; This issue is related to the relaxin hormone, which prevents premature contractions and may prevent the formation of scar tissue. But you must remember, pregnancy should not be considered as a treatment for disease relapses.
The effects of IBD on pregnancy, childbirth and fetus:
Usually, women with inflammatory bowel disease have a healthy pregnancy; But pregnancy complications such as miscarriage, premature birth and problems in childbirth may occur a little more than women without IBD. All women with IBD should receive the same special care as high-risk women.
IBD medications during pregnancy:
In most cases, the medication schedule before and during pregnancy remains the same and must be followed very carefully. The most dangerous thing is to stop taking medicines during pregnancy due to the fear of drug side effects, which can cause serious problems and even the death of the mother and the fetus. Of course, if the patient's condition changes, the dose or type of medicine may change. Summary of commonly used drugs:
Aminosalicylate (5-ASA):
eg Sulfasalazine and compounds like Mezalazine, these drugs do not have many side effects and do not harm the fetus; They may only cause nausea or heartburn. Due to the reduction of folic acid absorption, women should consume at least 2 mg of folic acid daily and can breastfeed while taking these drugs. data-generated-css="brz-css-czvwl">prednisolone and other steroids in most cases do not pose a particular risk during pregnancy; But in early pregnancy, it is preferable to reduce their dose. Infants
breastfed from mothers taking moderate to high doses of steroids should be monitored by a pediatrician.
Immunomodulators (immune system suppressors):
Drugs such as azathioprine and mercaptopurine (6-MP) should be continued in standard doses for pregnancy
> data-generated-css="brz-css-ljptv"> Both sexes (men and women) should avoid taking Methotrexate from three to six months before pregnancy. data-uniq-id="wdthf" data-generated-css="brz-css-ydrhs">Biological drugs:such as Infliximab, Adalimumab, which are used for Crohn's disease and Ulcerative colitis patients. These drugs are usually low-risk and do not appear in breast milk and must be continued.
Antibiotics:
If possible, it is better to avoid unnecessary antibiotics during pregnancy. Unless prescribed by a doctor, which are prescribed at the right time.
Diagnosis methods during pregnancy:
Safety methods such as Colonoscopy, sigmoidoscopy, endoscopy, rectal biopsy and abdominal ultrasound can be performed without risk during pregnancy. However, CT scan and standard X-ray are only used in emergency situations. MRI is also usually safe; Just avoid using gadolinium in the first trimester.
Surgery effects before and during pregnancy:
Removal of the small intestine before pregnancy usually does not have a negative effect on fertility. Women can have a successful pregnancy after ileoanal anastomosis (connection of the small intestine to the anus). Women who have a J pouch ileostomy may have lower fertility; Therefore, if possible, consult with your doctor at the IBD specialized center about the best timing of the operation.
Women who have had an ileostomy operation in the past may experience problems during pregnancy; Waiting for a year after the operation can reduce this risk.
Women who have a fistula or abscess around the anus or vagina usually have a cesarean section.
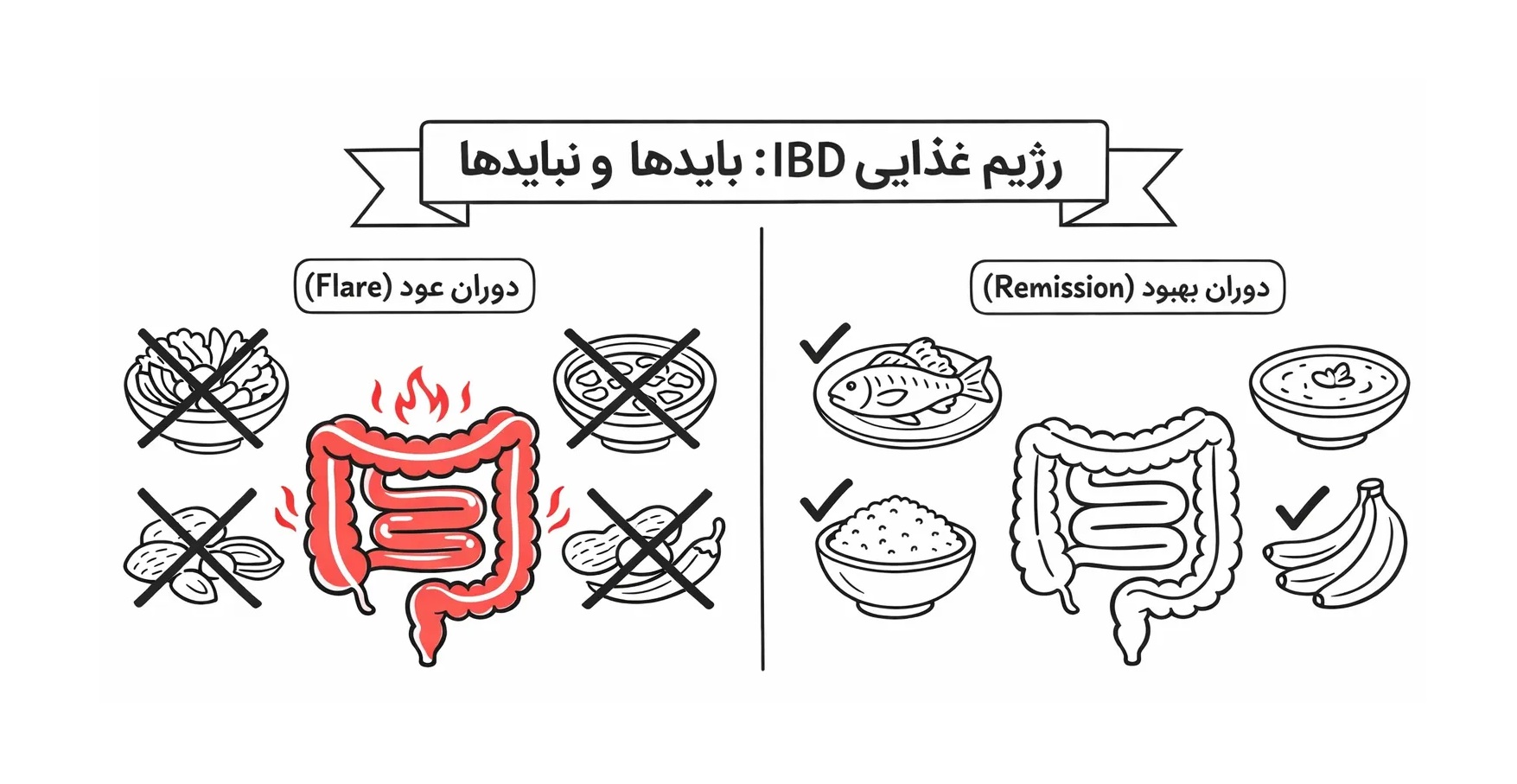
Nutritional needs during pregnancy:
All pregnant women, including women with inflammatory bowel disease, must have a proper diet. Taking vitamins, especially folic acid (at least 2 mg daily) is very important; Because it prevents birth defects such as spina bifida. This point is especially important for women who use Sulfasalazine.
Transmission of ulcerative colitis or Crohn's disease to children:
If one of the parents has IBD, the probability that the child will also get this disease is between 2 and 9%; So this possibility is very low.
With the cooperation of specialists at the IBD Center and the benefit of Advancing Crohn's & Colitis Care under the supervision of Dr. Ali Reza
Sima), you can experience a healthy and successful pregnancy with sufficient information and careful planning. Always remember that talking to an IBD Specialist is the key to success in managing Crohn's disease and Ulcerative Colitis. Healthy. Be!