Bite malocclusion or malocclusion is one of the most common dental problems in children that can negatively affect their oral health, chewing performance, speech and self-confidence. According to the guidelines of the American Association of Pediatric Dentistry (AAPD) and the National Institute of Dental and Craniofacial Research (NIDCR), prevention of malocclusion in children can reduce the need for complex orthodontic treatments by 60%. These anomalies, including crowding, openbite, crossbite, and class II and III malocclusion, are seen in 20 to 30% of children and have a similar prevalence in Iran. This article aims to provide specialized solutions for the treatment of jaw and teeth abnormalities in children, helping parents and professionals to design an effective program for children's mouth and jaw health. class="ez-toc-title-container">
anomaly What is an overbite and why is it important to prevent it?
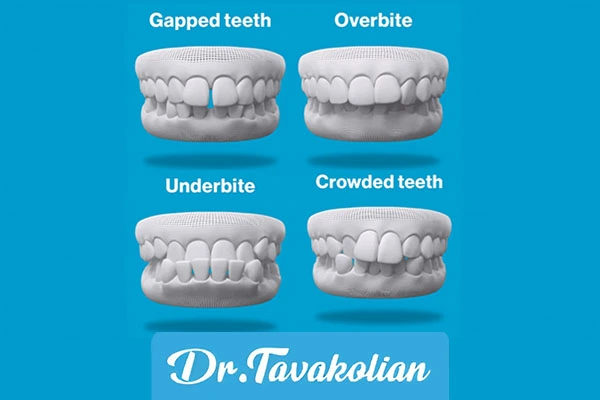
Bite abnormalities refer to improper alignment of the teeth and jaws, such as an open bite, cross bite, or excessive overjet. According to the NIDCR, this problem is more common in children ages 6 to 12 and can lead to childhood speech bite abnormalities, difficulty chewing, and cosmetic issues. The AAPD emphasizes that malocclusion is not only an appearance problem, but also increases the risk of tooth decay and gum disease because misaligned teeth are harder to clean. In Iran, about 25% of urban children suffer from moderate to severe malocclusion, which can be managed by preventing bite malocclusion in children.
The main causes of bite malocclusion include genetic factors (such as small jaw size), incorrect oral habits (long-term finger or pacifier sucking) and early loss of milk teeth. The AAPD reports that losing a baby tooth before age 8 increases the risk of a malformed bite by 40 percent. Choosing a specialist pediatric dentist, like Dr. Elham Tavaklian, can help prevent and treat jaw and teeth abnormalities in children.
treatment Jaw and teeth abnormalities in children
AAPD and NIDCR divide malocclusion risk factors into three categories:
Genetic: small jaw size or inherited craniofacial abnormalities, such as Rare syndromes.
Behavioral: incorrect habits such as finger sucking (in 30% of children up to 4 years old), mouth breathing due to allergies or nasal obstruction, and tongue pressure.
Dental: early childhood caries (ECC), early loss of baby teeth or delayed eruption of permanent teeth.
NIDCR studies show that children who continue to suck their fingers after age 4 are 50% more likely to develop open bites. A high-sugar diet that leads to ECC increases the risk of tooth loss and bite malformations. In Iran, with a 25% prevalence of ECC, it is important to pay attention to these factors for treatment of open bite in children with non-invasive methods.
Diagnosis methods of malocclusion in children is one of the most important steps in prevention and treatment. AAPD recommends that children undergo an orthodontic evaluation beginning at age 6, when the first permanent molar erupts. This evaluation is done using panoramic images, cephalometry and intraoral scanners. The Orthodontic Risk Assessment (ORA) tool is also used to identify oral habits and risk factors. NIDCR reports that early detection can reduce the need for orthodontic braces by 35 percent. Pediatric dentists, such as Dr. Elham Tavaklian, can detect abnormalities in time by using these diagnostic methods.
Incorrect oral habits such as long-term finger or pacifier sucking and mouth breathing are the main causes of bite abnormalities. The AAPD recommends Habit-Breaking Programs, which have an 80% success rate with positive methods such as rewards. For management of mouth breathing, referral to an otolaryngologist for nasal obstruction (such as enlarged adenoid) is necessary. The NIDCR reports that untreated mouth breathing increases the risk of Class II malocclusion by 45%. These non-invasive interventions can help treat children's open bite with non-invasive methods.
Methods for diagnosing malocclusion in children
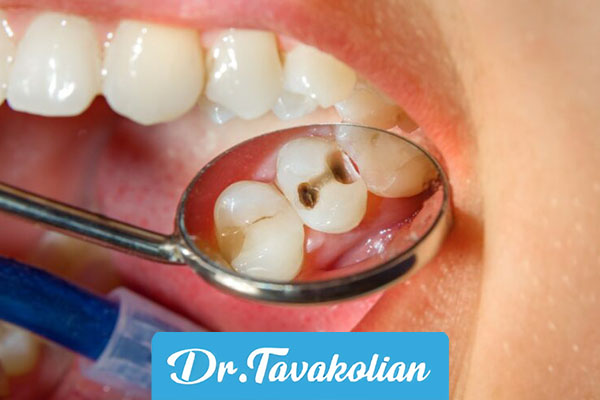
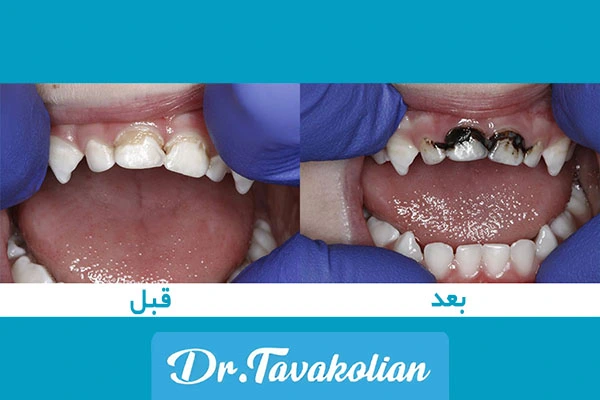
Maintaining the health of primary teeth plays a key role in preventing malocclusion with spacers in children. Early childhood caries (ECC) can lead to early loss of baby teeth, which increases the risk of tooth displacement and bite malformations. The AAPD recommends the use of silver diamine fluoride (SDF) for caries prevention. This material reduces the risk of early tooth loss by 77%.
In cases where milk teeth are lost, the use of spacers prevents the movement of adjacent teeth. NIDCR reports a 90 percent success rate for spacers. Specialist pediatric dentists can prevent malocclusion by using these tools.
Clinical studies confirm the effectiveness of early interventions. In a trial of 150 children, the use of spacers and weaning programs reduced the need for fixed braces from 60% to 25%. NIDCR also recommends the use of functional devices such as Myofunctional Appliances for children aged 7 to 10 years. These devices improve class II malocclusion by 50% by guiding jaw growth. In Iran, there are challenges such as limited access to orthodontists in rural areas, but free screening programs in schools can reduce the prevalence of malocclusion by 20%. href="https://dreltavakolian.ir/wp-content/uploads/2025/10/%D8%B9%D9%88%D8%A7%D8%B1%D8%B6-%D9%86%D8%A7%D9%87%D9%86%D8%AC%D8%A7% data-lazyloaded="1" src="data:image/svg+xml;base64,PHN2ZyB4bWxucz0iaHR0cDovL3d3dy53My5vcmcvMjAwMC9zdmciIHdpZHRoPSI2MDAiIGhlaWdodD0iNDAwIiB2aWV3Qm94P SIwIDAgNjAwIDQwMCI+PHJlY3Qgd2lkdGg9IjEwMCUiIGhlaWdodD0iMTAwJSIgc3R5bGU9ImZpbGw6I2NmZDRkYjtmaWxsLW9wYWNpdHk6IDAuMTsiLz48L3N2Zz4=" loading="lazy" decoding="async" class="size-full wp-image-6321" data-src="https://dreltavakolian.ir/wp-content/uploads/2025/10/Awarz-Nahanjari-Bayt-der-Govtar-Kodekan.webp" alt="Awarz-Nahanjari Bait-Der-Govtar-Kodekan.webp" alt="Awarz Nahanjari Bait-Der-Govtar-Kodekan.webp" alt="Awarz Nahanjari Bait in Children's Speech" width="600" height="400" data-srcset="https://dreltavakolian.ir/wp-content/uploads/2025/10/Awarz-nahanjari-bayt-der-govtar-kodkan.webp 600w, https://dreltavakolian.ir/wp-content/uploads/2025/10/Awarz-anhamjari-byte-der-govtar-kodkan-272x182.webp 272w" data-sizes="auto, (max-width: 600px) 100vw, 600px">Awarz Byte anomaly in children's speech
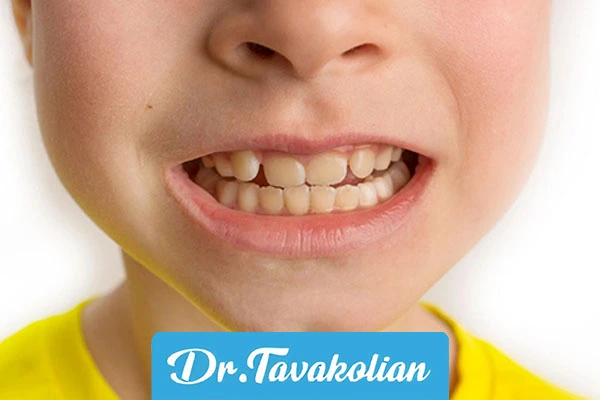
Bite malocclusion or malocclusion in children can cause significant speech complications, including defects in the pronunciation of sounds, reduced speech clarity, and difficulties in pronouncing certain letters such as "s", "sh" and "t". These problems occur due to misalignment of the teeth and jaws, such as an openbite or crossbite, which disrupts the coordination of the tongue, lips, and palate. According to the NIDCR report, about 20-30% of children with moderate to severe malocclusion have speech disorders that can reduce their confidence in social communication. Early interventions, such asPreventive orthodontics in childrenFrom the age of 6, using spacers and giving up bad oral habits under the guidance of experts like Dr. Elham Tavaklian can minimize these complications and improve the child's speech and oral health.
Parents should pay attention to their child's oral habits from the age of 3 and start regular dental visits from 6 months. A low-sugar diet and quitting bad habits can reduce the risk of bite abnormalities by 30%. In Iran, cultural acceptance of long-term pacifiers can be addressed with targeted educational programs. Pediatric dental professionals should use modern diagnostic tools such as CBCT and AAPD protocols for early intervention. Collaboration with speech therapists and ENT specialists is also necessary to manage the effects of byte abnormalities in children's speech.
Bayt Anomaly>
Bite malformation prevention in children is possible with early screening, leaving oral habits and preserving milk teeth. This approach not only reduces treatment costs, but also improves the oral health and quality of life of children. Parents are encouraged to consult pediatric dentists, such as Dr. Elham Tavaklian, and take advantage of AAPD and NIDCR resources. For more information and to receive specialized services, contact Dr. Elham Tavaklian's office.
Words Key: prevention of malocclusion in children, treatment of malocclusion in children, prevention of malocclusion with spacers in children, treatment of open bite in children with non-invasive methods, methods of diagnosis of malocclusion in children, complications of bite malocclusion in children's speech

 Treatment of open bite in children with non-invasive methods
Treatment of open bite in children with non-invasive methods